To review the full Recordati Rare Diseases Canada Inc. Privacy Policy,
please click here.
By following this link you will be leaving PANHEMATIN.ca for another
Recordati website. Please note that this website may not be appropriate
for all audiences.
×
Terms of Use
To review the full Recordati Rare Diseases Canada Inc. Terms of Use,
please click here.
By following this link you will be leaving PANHEMATIN.ca for another
Recordati website. Please note that this website may not be appropriate
for all audiences.
Exiting to External Site
You are about to leave the PANHEMATIN.ca website and enter a
website operated by an independent third party. The links to third-party
websites contained on PANHEMATIN.ca are provided solely for your
convenience. Recordati Rare Diseases Canada does not control the
opinions, claims, or comments contained on any third-party website
linked to PANHEMATIN.ca. Your activities at those websites will be
governed by the policies and practices of those third parties.
Exiting to External Site
You are about to leave the PANHEMATIN.ca website and enter a
website operated by an independent third party. The links to third-party
websites contained on PANHEMATIN.ca are provided solely for your
convenience. Recordati Rare Diseases Canada does not control the
opinions, claims, or comments contained on any third-party website
linked to PANHEMATIN.ca. Your activities at those websites will be
governed by the policies and practices of those third parties.
X
How to order PANHEMATIN
Order through Canadian Blood Services and Héma‑Québec
PANHEMATIN is supplied as a sterile, lyophilized black powder in single dose dispensing vials in a carton.
The vial stopper contains natural rubber latex.
Store lyophilized powder at 20-25°C (68-77°F).
PANHEMATIN summary of chemical and clinical response
Chemical and clinical response to the treatment of AIP attacks was assessed in 72 patients.1,†
Summary of clinical and chemical response data from PANHEMATIN open-label studies1
Investigator/publication
AIP patients
Treatment courses
Dose
Other treatments prior to PANHEMATIN
Chemical response†
Clinical response†
Watson CJ et al1,2
11
13
4 mg/kg/day or 4 mg/kg 2x/day for 1 to 4 days‡
Glucose
58-100% reduction in serum ALA & PBG levels (11/11 patients)
91% (10/11 patients)
Pierach CA et al1,3
43
82
2-4 mg/kg/day
...§
For those patients with elevated urinary ALA & PBG levels prior to treatment
90% (74/82 treatment courses)
Lamon JM et al1,4
11
20
~2-4 mg/kg/day or 2-4 mg/kg 2x/day for 3 to 13 days‡
High carbohydrate intake
Significant reductions in ALA and/or PBG levels (p<0.001 to 0.05) (11/11 patients)
70% (14/20 treatment courses)
McColl KE et al1,5
7
12
4 mg/kg/day or 4 mg/kg 2x/day for 3 to 5 days‡
...§
50% reduction in urinary ALA and PBG levels from pre-treatment values (7/7 patients)
58% (7/12 treatment courses)
Lamon JM et al1,6,II
7¶
11
1 mg/kg every 24 hours for 3 to 13 days
250-300 g/24 h carbohydrate diet
Decrease in ALA and PBG occurred in every patient (except one PBG value in one patient) when treatment lasted 5 days or longer (p<0.001)
...
Investigator/publication
Watson CJ et al1,2
Pierach CA et al1,3
AIPpatients
11
43
Treatmentcourses
13
82
Dose
4 mg/kg/day or 4 mg/kg 2x/day for 1 to 4 days‡
2-4 mg/kg/day
Othertreatmentsprior toPANHEMATIN
Glucose
...§
Chemicalresponse†
58-100% reduction in serum ALA & PBG levels (11/11 patients)
For those patients with elevated urinary ALA & PBG levels prior to treatment
Clinicalresponse†
91% (10/11 patients)
90% (74/82 treatment courses)
Investigator/publication
Lamon JMet al1,4
McColl KEet al1,5
AIP patients
11
7
Treatmentcourses
20
12
Dose
~2-4 mg/kg/day or2-4 mg/kg/ 2x/day for 3 to 13 days‡
4 mg/kg/day or4 mg/kg2x/day for 3 to 5 days‡
Othertreatmentsprior toPANHEMATIN
High carbohydrate intake
...§
Chemicalresponse†
Significant reductions in ALA and/or PBG levels (p<0.001 to 0.05) (11/11 patients)
50% reduction in urinary ALA and PBG levels from pre-treatment values (7/7 patients)
Clinicalresponse†
70% (14/20 treatment courses)
58% (7/12 treatment courses)
Investigator/publication
Lamon JM et al1,6,II
AIPpatients
7¶
Treatmentcourses
11
Dose
1 mg/kg every 24 hours for 3 to 13 days
Othertreatmentsprior toPANHEMATIN
250-300 g/24 h carbohydrate diet
Chemicalresponse†
Decrease in ALA and PBG occurred in every patient (except one PBG value in one patient) when treatment lasted 5 days or longer (p < 0.001)
Clinicalresponse†
...
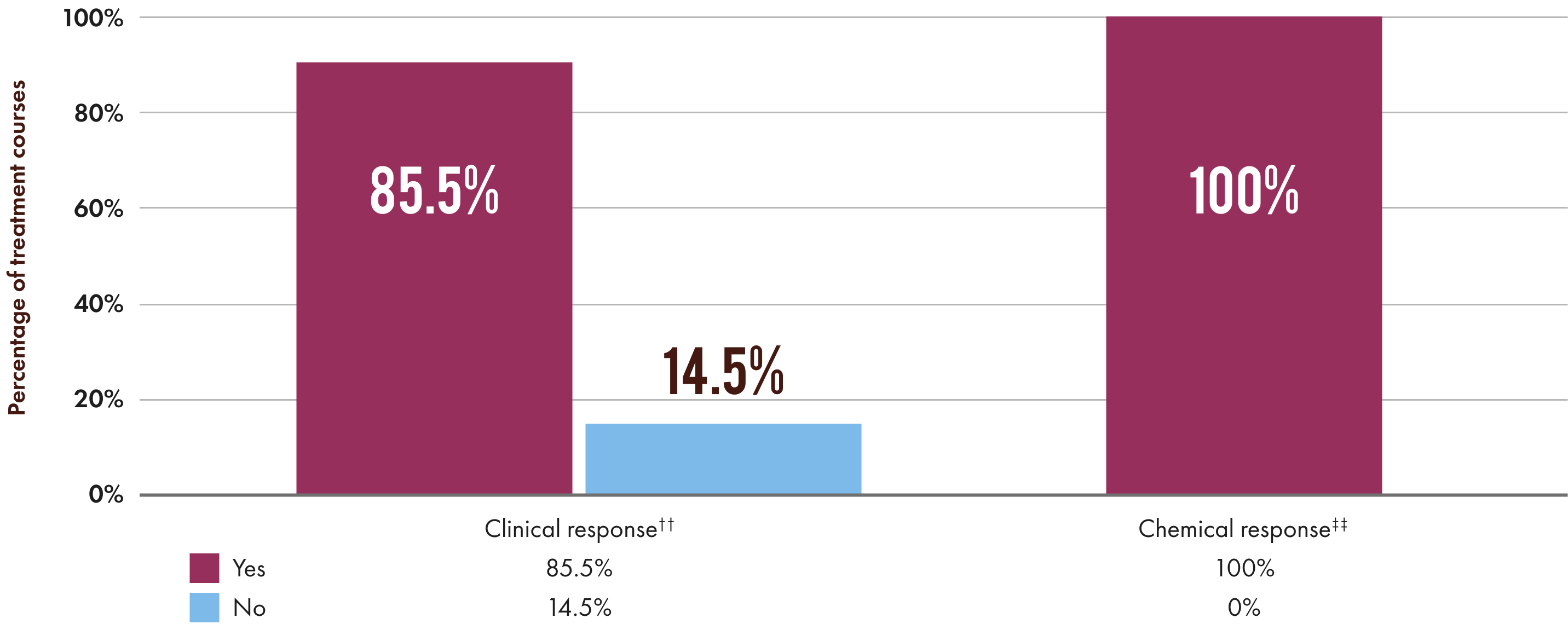
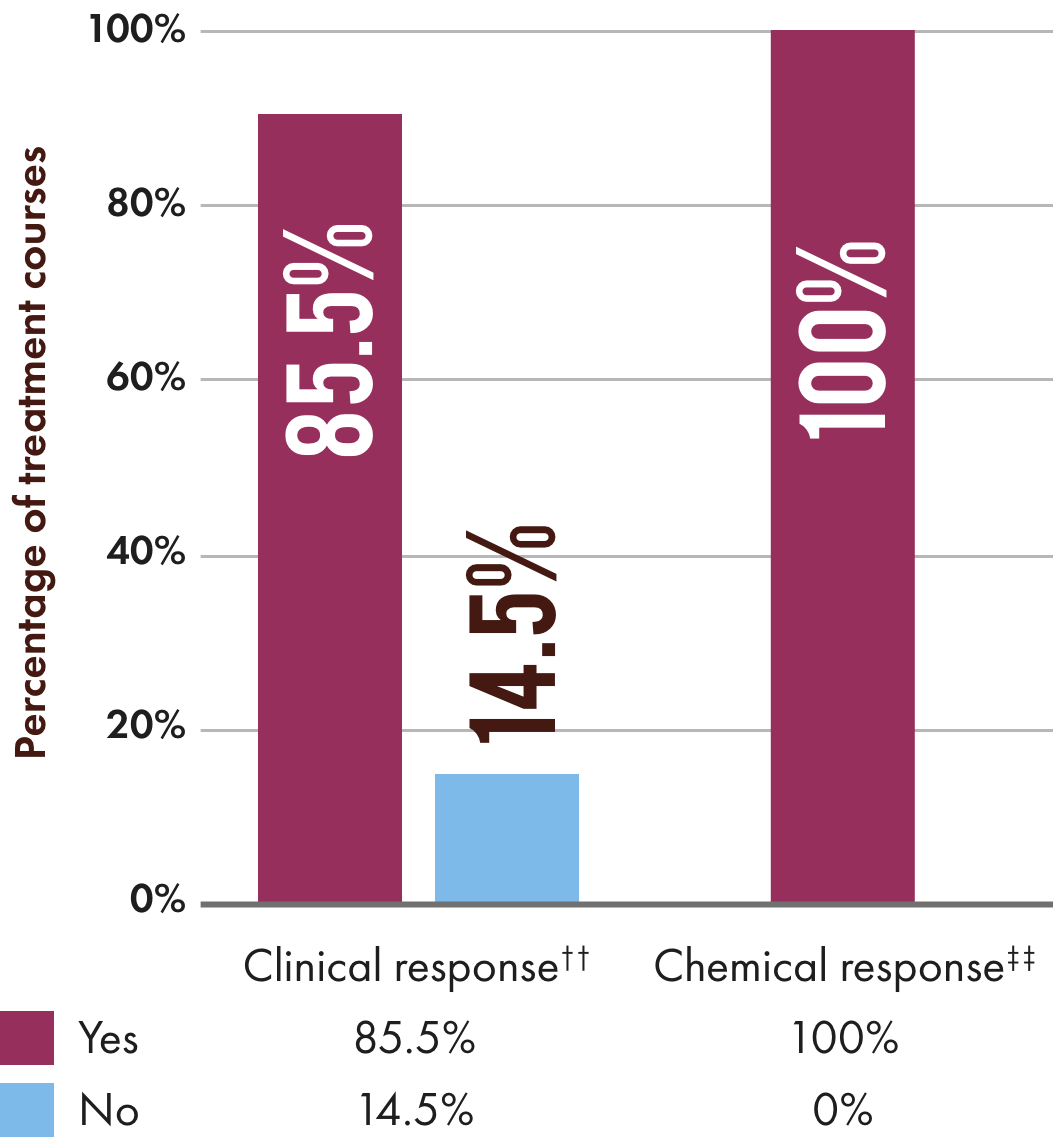
PANHEMATIN efficacy data from 5 open-label studies
Patients experienced a clinical response†† in 85.5% (141/165) of treatment courses (open-label trials).1
73% (81/111) of patients achieved clinical response for all acute attacks‖‖85% (94/111) of patients had ≥1 clinical response and 15% (17/111) had no response
Observational study with patient-reported outcomes1,8
90
55% (50/90) reported receiving hemin during acute attacksOf these patients,74% (37/50) reported PANHEMATIN as being very successful in treatment of abdominal pain and other symptoms. Hemin therapy effectiveness was assessed along with glucose infusions, high carbohydrate diets, and pain medications on a scale from zero being least effective to 10 highly effective. Hemin infusions received a 7.9, glucose infusions a 4.4 (p=0.0781), high carbohydrate diets a 4.7 (p=0.0021), and pain medications a 4.2 (p=0.0049).
† Chemical and clinical responses were individually defined by each investigator in each study.
‡ The dose of PANHEMATIN is 0.8 to 3.1 mg/kg/day of hematin for 3 to 14 days based on the clinical signs. The standard dose in clinical practice is 2.3 to 3.1 mg/kg/day. In more severe cases this dose may be repeated no earlier than every 12 hours. Do not exceed 4.6 mg/kg of hematin in any 24-hour period.
§ PANHEMATIN is indicated for the amelioration of recurrent attacks of acute intermittent porphyria (AIP) temporally related to the menstrual cycle in susceptible women, after initial carbohydrate therapy is known or suspected to be inadequate.
II Clinical response in Lamon et al (1977) was not evaluated.
¶ Seven patients with acute attacks of porphyria. AIP not specified.
†† Clinical response defined as improvement of symptoms and reduction in pain.
‡‡ Chemical response defined as normalization of urinary aminolevulinic acid (ALA) and porphobilinogen (PBG).
§§ 90 patients were treated for acute attacks and 21 patients for both acute attacks and prophylaxis. PANHEMATIN is not indicated for prophylaxis.
‖‖ Clinical response was achieved if the physician determined that the admitting symptoms were resolved, there was a clinically acceptable response, or the patient went into remission.
References
Recordati Rare Diseases Canada Inc. PANHEMATIN Product Monograph. July 13, 2018.
Watson CJ, Pierach CA, Bossenmaier I, et al. Hematin in “inducible” hepatic porphyrias. Adv Intern Med. 1978;265-286.
Pierach CA, Bossenmaier I, Cardinal R, et al. Hematin therapy in porphyric attacks. Klin Wochenschr. 1980;829-832.
Lamon J, Frykholm B, Hess R, et al. Hematin therapy for acute porphyria. Medicine (Baltimore). 1979;252-269.
McColl KEL, Moore MR, Thompson GG, et al. Treatment with haematin in acute hepatic porphyria. Q J Med. 1981;161-174.
Anderson KE, Collins S. Open-label study of hemin for acute porphyria: clinical practice implications. Am J Med. 2006;119(9):19-24.
Bonkovsky HL, Maddukuri VC, Yazici C, et al. Acute porphyrias in the USA: features of 108 subjects from porphyrias consortium. Am J Med. 2014;127(12):1233-1241.
PrPANHEMATIN® (hemin for injection) is indicated for the amelioration of recurrent attacks of acute intermittent porphyria temporally related to the menstrual cycle in susceptible women, after initial carbohydrate therapy is known or suspected to be inadequate.
Limitations of use:
Before administering PANHEMATIN, consider an appropriate period of carbohydrate loading (i.e., 400 g glucose/day for 1 to 2 days).
Indication:
PrPANHEMATIN® (hemin for injection) is indicated for the amelioration of recurrent attacks of acute intermittent porphyria temporally related to the menstrual cycle in susceptible women, after initial carbohydrate therapy is known or suspected to be inadequate.
Limitations of use:
Before administering PANHEMATIN, consider an appropriate period of carbohydrate loading (i.e., 400 g glucose/day for 1 to 2 days).
Attacks of porphyria may progress to a point where irreversible neuronal damage has occurred. PANHEMATIN therapy is intended to prevent an attack from reaching the critical stage of neuronal degeneration. PANHEMATIN is not effective in repairing neuronal damage.
Clinical use:
Pediatrics (<16 years of age): Based on the data submitted and reviewed by Health Canada, the safety and efficacy of PANHEMATIN in pediatric patients has not been established; therefore, Health Canada has not authorized an indication for pediatric use.
Geriatrics (≥65 years of age): Clinical data for subjects aged 65 and over was not sufficient to determine whether they respond differently from younger subjects. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Contraindications:
PANHEMATIN is contraindicated in patients who are hypersensitive to this drug or to any ingredient in the formulation, including any non-medicinal ingredient, or component of the container.
Relevant warnings and precautions:
Risk of phlebitis.
Risk of transmitting infectious agents (e.g., viruses, the variant Creutzfeldt-Jacob disease (vCJD) agent, and theoretically the Creutzfeldt-Jacob disease (CJD) agent).
Transient, mild anticoagulant effects may occur. Avoid concurrent anticoagulant therapy.
Elevated iron and serum ferritin may occur. Monitor iron and serum ferritin in patients receiving multiple administrations of PANHEMATIN.
Reversible renal shutdown has been observed in a case where an excessive hematin dose (12.2 mg/kg) was administered in a single infusion. Recommended dosage guidelines should be strictly followed.
Should be given to a pregnant woman only if clearly needed. Avoid administering hematin in severe pre-eclampsia.
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for PANHEMATIN and any potential adverse effects on the breastfed child from PANHEMATIN or from the underlying maternal condition.
Avoid CYP inducing drugs (such as estrogens, barbituric acid derivatives, and steroid metabolites) while on PANHEMATIN therapy.
By following this link, you will be leaving www.panhematin.ca for another Recordati website. Please note that this website may not be appropriate for all audiences.
Exiting to a third-party website
By following this link, you will be leaving a Recordati-controlled website for a third-party website. Please note that Recordati is not responsible or liable for any third-party website and the website may not be appropriate for all audiences.
Pursuant to the legislation applicable to the protection of personal data (“Privacy Legislation”) including EU Regulation 2016/679 (“GDPR”) as well as the supervisory authorities’ measures on cookies, Recordati Industria Chimica e Farmaceutica S.p.A provides users (hereinafter the “Users” or in the singular, the “User”) with the following information regarding cookies installed on the following domain [www.panhematin.ca] (the “Website”).
Who is the Data Controller?
The Data Controller is Recordati Industria Chimica e Farmaceutica S.p.A. parent company of the Recordati Group, with registered office in Milano, Via M. Civitali n. 1, enrolled in the Register of Companies of Milan under number 00748210150 (hereinafter, the “Company”, the “Data Controller” or “Recordati“).
The Data Protection Officer of the Recordati Group (hereinafter, the “DPO”) can be contacted at the following e-mail address: groupDPO@recordati.com.
What are cookies?
Cookies are text files and numbers that are installed while browsing on a website, in the memory of the device (PC, smartphone or tablet) connected to the Internet through the browser application installed therein.
Cookies, which are usually present in substantial numbers in users’ browsers and sometimes also with wide temporal persistence, are used for several purposes such as, by way of example and not limited to, for IT authentication, for monitoring of browsing sessions, for storage of information on specific user configurations in accessing a given server, etc.
The Privacy Legislation identifies the following macro-categories of cookies:
“Technical cookies”, which are used to carry out browsing or to provide a service requested by the user. Such cookies are not used for further purposes and are usually installed directly by the website’s owner or manager. In addition, these cookies can be grouped into:
browsing or session cookies, which guarantee the normal browsing and use of a website (allowing, for example, to purchase items online or authenticate to access certain sections);
functional cookies, which allow users to navigate as a function of certain pre-determined criteria (such as, for example, language, products selected for purchase) in order to improve the quality of service provided to the same. For the installation of technical cookies, the users’ prior consent is not necessary;
“Analytics cookies”, which are used to monitor the use of a website by users for optimization purposes (number of visitors, pages browsed, time spent on a website, etc.).
In order for analytics cookies to be equated to technical cookies, it is necessary that they are realized and used directly by the first party website (without the intervention of third parties) to improve its usability and it is necessary to prevent the possibility that, through their use, direct identification of data subjects is achieved, which is tantamount to preventing the use of analytics cookies that, due to their characteristics, can work as direct, unique identifiers of users.
In order to consider analytics cookies, including third-party cookies, as technical cookies, it is necessary that: (i) analytics cookies are only used for the production of aggregated statistics and in relation to a single website or a single mobile application, so as not to allow tracking an individual’s navigation across different applications or websites; (ii) at least, for third-party analytics cookies, the fourth component of the IP address is masked out; (iii) the third parties refrain from match such analytics cookies with any other information (such as customer records or statistics concerning visits to other websites) or from forwarding them to third parties.
For the installation of analytics cookies which can be assimilated to technical cookies, the users’ prior consent is not required; where, however, analytics cookies cannot be assimilated to technical cookies, the users’ consent to their installation is then required;
“Profiling cookie”, which are intended to create user’s profiles and are used to send targeted advertising messages in line with the preferences expressed by the user in the context of his/her web-browsing activities. Due to the particular invasiveness that these cookies may have on the private sphere of the users, the Privacy Legislation provides that user shall be adequately informed about the use of such cookies and express his/her valid consent for the installation of the same. For the installation of profiling cookies, the users’ prior consent is therefore necessary, which should be provided after the user has been informed in a simplified manner;
Moreover, cookies may be installed directly by the website visited by the user (s.c. “first-party cookies”), or they may be installed by other websites (s.c. “third-party cookies”).
Lastly, under the temporal prospective, cookies can be divided into: (i) “persistent cookies”, i.e. cookies that are permanently stored on the user’s device until a predetermined expiry date (minutes, days, years); (ii) “session cookies”, i.e. cookies that are automatically deleted when closing the browser.
What cookies does the Website use and for what purposes?
When the User connects to the Website, the following cookies may be installed on the User’s device:
(i) Technical cookies
These cookies are necessary in order to allow the operation of the Website and cannot be deactivated within the Company's systems. They are usually set only in response to actions taken by the User that constitute a service request, such as setting privacy preferences, logging in, or filling out forms. It is possible to set the browser so that it blocks these cookies but, as a result, some parts of the Website will not work properly. These cookies do not store any personal data.
Technical cookies
Cookie name
Domain
Type
Duration
Purposes
How to deselect
panhematin-DIN
www.panhematin.ca
First-party cookie
8 hours
Authentication cookie used to evaluate whether user has entered the proper password to access the site content.
N/A
panhematin-cookie-agreed
www.panhematin.ca
First-party cookie
Forever
Used to save the website store when the user has accepted the cookie policy and to not show the banner for future visits.
N/A
(i) First and third-party analytics cookies that can be assimilated to technical cookies
These first-party and third-party cookies, as far as they can be assimilated to technical cookies, allow the Company to count visits and traffic sources so that it can measure and improve the performance of the Website. They help the Company knowing which pages are the most and least popular and see how visitors navigate around the Website. All information collected by cookies is aggregate and therefore anonymous.
Analytics cookies
Cookie name
Domain
Type
Duration
Purposes
How to deselect
_ga_*, __gid_*, __gat_*, __pk_*
www.panhematin.ca
Third-party cookie
1 year
Anonymous analysis of visits and browsing performance.
For further information, please refer to the third party's privacy notice here: https://policies.google.com/technologies/cookies?hl=it&gl=it.
N/A
Please note that:
first-party cookies are under the direct and exclusive responsibility of the Data Controller;
third-party cookies are under the direct and exclusive responsibility of the third party itself.
It follows that third party cookie providers are also required to comply with the Privacy Legislation. For this reason, the Users shall refer to the links to the third party’s webpages, where they can find the third party’s cookie consent forms (where necessary) and the related privacy notice.
How can the User manage and/or deactivate cookies?
When the User visits the Website for the first time, he/she will be informed about the type of cookies used by the Website by means of an information banner that appears immediately at the top of the Website. Following the display of the banner, by continuing to browse the Website, the User accepts the use of cookies selected by the Website (such as, for example, technical cookies).
However, it is always possible to modify the cookie settings at any time by following the procedures outlined in this privacy notice.
How can the User manage his/her cookie preferences through the browser?
Each browser allows the User to limit and delete cookies. The User can manage cookie preferences directly in his/her browser and prevent - for example - the installation of third-party cookies.
Please find below the procedure to deactivate the cookies directly through the configuration settings of the main browser applications:
Internet Explorer
Open Internet Explorer;
click on the “Tools” button and then on “Internet Options”;
select the “Privacy” tab and move the slider to the level of privacy you wish to set (up to block all cookies or down to allow all cookies);
then click on “Ok”.
Google Chrome
Open Google Chrome;
click on the “Tools” button
select “Settings” and then “Advanced Settings”;
Select “Content Settings” under “Privacy” section;
In the "Cookies" tab it is possible to deselect cookies and save the preferences.
Firefox
Open Firefox;
click the "Alt" button on the keyboard;
in the toolbar at the top of the browser, select “Tools” and then “Options”;
then select the “Privacy” tab;
go to "Settings History" and then to “Use Custom Settings”;
deselect “Accept cookies from websites” and save the preferences.
Opera
Open Opera;
click on the “Settings” in the browser menu and select “Settings”;
select “Quick preferences”;
deselect “Enable cookies”.
Safari
Open Safari;
choose “Preferences” in the toolbar, and then select the “Safety” panel in the dialogue box that follows;
in the section “Accept Cookies”, you can specify if and when Safari must save cookies from websites. For further information, please click on the “Help” button (marked with a question mark);
for more information about cookies that are stored on your computer, click “Show Cookies”.
After these operations, however, some functions of the Website may not be performed and/or work properly.
With whom are the data collected by using cookies shared?
The data collected by using cookies may be processed by the Company's employees, in their capacity as authorized persons pursuant to the Privacy Legislation.
Such data may also be processed by companies which carry out technical and organizational activities on behalf of the Company, including IT consultants and web agencies which develop and manage the Recordati Group's websites and profiles on the social media in which Recordati is registered. These companies are direct collaborators of the Company and operate by virtue of a specific deed of appointment as data processors.
Personal data collected by using cookies will not be shared to third parties and will be processed exclusively within the European Union. Should the need to transfer data outside the European Union arise, the Company will ensure that such transfers are carried out only in presence of appropriate safeguards pursuant to Article 46 et seq. of the GDPR.
Data collected by using cookies will not be disseminated.
What rights can User exercise?
The User will always have, in accordance with the law, the right to withdraw at any time his/her consent, where given, as well as to exercise, at any time, the following rights:
the “right of access” i.e. the right to obtain confirmation as to whether or not personal data concerning the User are being processed and the communication of such data in an intelligible form;
the “right to rectification” i.e. the right to request the rectification or, if interested, the integration of personal data;
the “right to erasure” i.e. the right to request the erasure or the anonymization of personal data that have been processed unlawfully, including data whose storage is unnecessary for the purposes for which they were collected or further processed;
the “right to restriction of processing” i.e. the right to obtain from the Data Controller the limitation of the processing in certain cases provided for under the Privacy Legislation;
the right to request the Data Controller to indicate the recipients to whom it has notified any rectification or erasure or restriction of processing (carried out in accordance with Articles 16, 17 and 18 GDPR, in fulfillment of the notification obligation unless this proves impossible or involves disproportionate effort);
the “right to data portability” i.e. the right to receive (or transmit directly to another data controller) personal data in a structured, commonly used and machine-readable format;
the “right to object”, i.e. the right to object, in whole or in part:
the processing of personal data carried out by the Data Controller for its own legitimate interest;
the processing of personal data carried out by the Data Controller for direct marketing or profiling purposes.
In the above cases, where necessary, the Data Controller will inform the third parties to whom the User's personal data has been disclosed of the his/her exercise of rights, unless it is not possible or is too onerous and, in any case, in accordance with the provisions of the Privacy Legislation.
Where processing is based on consent, the User is also entitled to withdraw, at any time, any consent given, whereby it is understood that the withdrawal of consent shall not affect the lawfulness of the processing based on consent given prior to the withdrawal.
How to exercise your rights?
The User is entitled to exercise his/her rights at any time by using the contact details indicated in the section “Who is the Data Controller?“ above or by writing to the DPO by e-mail at the following address: groupDPO@recordati.com.
The Data Controller hereby informs the User that, pursuant to the Privacy Legislation, he/she has the right to lodge a complaint with the competent supervisory authority (in particular in the Member State of User’s habitual residence, place of work or place of the alleged breach), if he/she is of the opinion that his/her personal data are being processed in a way that would lead to breaches of the GDPR.
In order to facilitate the exercise of the right to lodge a complaint, the name and contact details of the European Union Supervisory Authority are available at the following link: https://ec.europa.eu/justice/article-29/structure/data-protection-authorities/index_en.htm.
This site uses cookies to provide you with a more responsive and personalized service. By using this site, you agree to our use of cookies as set out in our cookie policy. Please read our cookie policy for more information on the cookies we use and how to delete or block the use of cookies.